|
About Our Staff
About Therapy
Services
Neuropsychology
Neurocognitive
Rehabilitation
Health Psychology
Biofeedback
Neurofeedback
Pain Management
Stress Management
CBT
Policies
Office
Contact Us
Useful Sites
Home
| |
|
Neurocognitive Rehabilitation
Until relatively recently, most scientists and neurologists believed
that brain development occurred primarily in childhood and adolescence
and that functional areas of the brain, once developed, remained
relatively stable for the rest of an individual's life. Functions
lost as a result of an acquired brain injury could not be regained
beyond any improvement which might occur during a relatively short
recovery period. More recently, however, various lines of inquiry
have led to the conclusion that the brain can often reorganize itself
after an injury, a property referred to as plasticity. If an area
associated with a specific function is damaged, the brain may be
able to redevelop that function in a different, undamaged area.
|
|
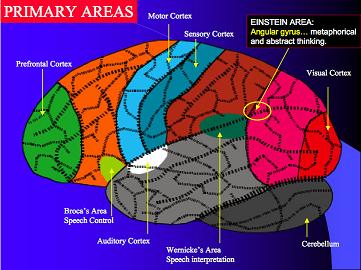
Distribution of functions in the brain is not as simple as diagrams
such as this one would indicate.
|
Many functions are actually distributed across multiple areas
within the brain and are not conveniently confined to specific
regions, and cognitive functions share pathways and brain structures,
so that a cognitive deficit isolated to memory, for example, without
accompanying deficits in other cognitive areas, is relatively uncommon.
In some instances the injury to the brain may be biochemical rather
than anatomic.
The discovery of plasticity has led to the concept that significant
improvement in cognitive functioning can be achieved after an insult
such as a stroke or traumatic brain injury by using various techniques
to encourage the brain to restructure itself in ways that will support
cognitive functions. These techniques are included in programs
referred to by terms such as neurocognitive rehabilitation. They
generally focus on processes such as attention, memory and executive
functions, which include skills such as planning, decision making,
time management, problem solving and mental flexibility. Cognitive
exercises have been shown to be effective in improving these abilities.
However, the focus of neurocognitive rehabilitation is somewhat
broader than this description might suggest, and is directed towards
the practical goal of helping the patient become as independent and
functional as possible; in addition to cognitive exercises, the
rehabilitation program will employ other techniques as appropriate,
such as teaching the use of various aids to memory (notebooks or
lists, for instance) to compensate for residual memory deficits.
Both the rehabilitation exercises and the compensatory techniques
may use computers or digital devices, so technological advances
are making significant contributions to cognitive rehabilitation.
|
